��ijij����61��
Mr.Jia, male, 61 years old
һ�������ص�
General Information
��ʷ
�ֲ�ʷ:
������3����ǰ��������������������ﲻ�壬���ۺ졢����У�����ʹ�����Ӽ�������Σ���Ӱ�ڵ����ڵ���ҽԺ��飬���Ϊ��Ĥ�ף�����ҩ����(���岻��)��֮����������ģ�����أ������Ϸ���Ӱ�ڵ�����������Ժ���������Ϊ��������Ĥ���룬Ϊ��һ����������Ժ��
����ʷ��
Ѫ��ƫ��2��
��ʪ�Թؽ���1�꣬��ҩ����
��������ȫ����
����ʷ��
����40֧/���40�꣬���ư��/���40��
����ʷ������
����ʷ��
���ϼ������Ŵ���ʷ
Medical History
Present Medical History:
The patient suffered from vision decrease in the right eye for three months. Initially, he had red eye and foreign body sensation without pain, distortion or vision block. He was diagnosed as conjunctivitis and administratedsome antibiotic eye drops in a local clinic, but the symptoms remained. The vision decreased gradually in the right eye, and vision block in superior visual field developed. He was admitted for further treatment options.
Past Medical History:
Hyperglycemia for 2 years.Rheumatoid arthritis for 1 year , currently on traditional Chinese medicine therapy
Personal History:
Smoking :40 Cigarettes/ day ��40 years.
Drinking :250g / day��40 years
Family history:
Unremarkable.
�۲����
���ۣ�
Vod 0.1��IOP 12.0mmHg��1�ⶨλ�����ϣ��Ϸ�������(-)�����(+)����״������»��ǣ�����������״���ǣ��۵�ģ������λ���·�4��-8��λ�ܱ߲�����Ĥ���������¡��;��λ���·�����Ĥ������ƽ��������Ĥ�����ۼ��ư�;��Ϸ�Զ�ܱ߲��ɼ�һԲ��¡��
���ۣ�
Vos 0.6 ��IOP 14.7mmHg����״���������죬����������״���ǣ��۵ף����̽���ɫ����C/D 0.7���ư���δ�������쳣���ܱ�����Ĥδ�����롣
Ocular examinations
Right eye:
Vod 0.1, IOP 12.0mmHg. A superior visual field defect, subcapasular opacity of the lens, and mild vitreous opacity were noticed Fundusexamination in upright position found bullous retinal detachment at 4-8o��clock in the peripheral portion of the retina, whereas in the supine positionthe retinal detachment shifted to the posterior part of the retina involving the macular. No retinal hole was found. A protuberant lesion was noticed in the temporal-superiorquadrant of the peripheral retina.
Left eye:
Vos 0.6, IOP 14.7mmHg. There was subcapasular opacity of the lens and mild vitreous opacity. The C/D ratio was 0.7. No significant abnormality was found.
�������
Accessory Examination:
ͼ1 ���۲�ɫ�۵�ͼ��
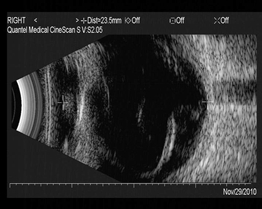
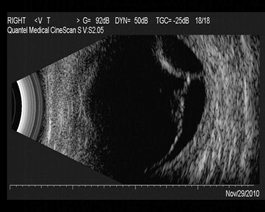
ͼ2 B������������Ĥ���룬����Ĥ����?
Fig 2 B- scan showed retinal detachment in the right eye, and choroidal detachment was suspected in the temporal-superior part.
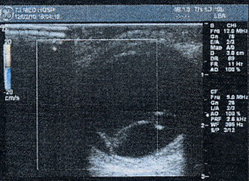
ͼ3 CDI�����۲�����ǻ�ڿɼ�Y�ε�������ͷ����¡�����������ڿɼ�����ɫѪ���źš���Ϸ��ɼ���Բ��¡�𣬻���20.75px����12px���߽�������ڲ�������δ̽������Ѫ���źż������źţ�¡�����ɼ�Ѫ���źţ����¡���ڻ���Ե������
Fig3 CDI showed a Y-shapedstrip with rich blood supply connecting to the optic papilla. In the temporal region. There was a semicircular bulge with a base of 20.75px��12px.Blood flow signals were not visible on the surface of the bulge, and was continuous with the uplift of the posterior pole at the base margin.
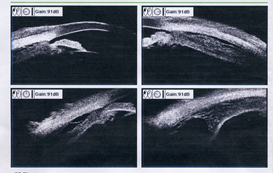
ͼ4 UBM��ǰ���������1.94mm��ȫ��С����Ĥ�нǿ��ţ�ȫ�ܽ�״��ˮ�����룬��Ϸ���״����ϴ���ǻ��������.
Fig 4 UBM showed circumferential ciliary body edema and a localized ciliary cyst in the temporal-superior part. No echo sound was detected inthe cavity.
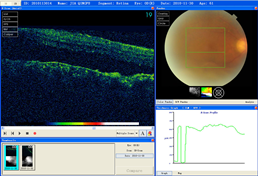
ͼ5 OCT�����ۻư�ɫ����Ƥ���䣬����Ƥ����
Fig5 OCT revealed RPEirregularity in the macula and retinal detachment.

ͼ6����Ӱ����
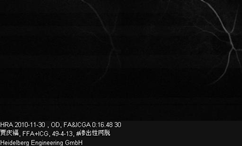
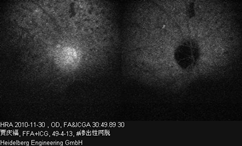
���ۣ�FFA����������ӯʱ�����ӳ٣�������Χ�������ư���ΧѪ�ܹ������ɼ�������С��Բ�Σ����ε�ӫ��ߣ��߽������������ںϳ�Ƭ����ʱ���ӳ�����ӫ�����δ����Ⱦ�����̱߽粻�壬���Բ����ӫ�⣬�߽�������·���ĤѪ��Ư��(����)�����ڣ�����ǿӫ�⣬���Բ����ӫ�����ǿӫ�⣬ICGA����Ӧ��λʼ����Բ�ε�ӫ�⣬�����ޱ仯��
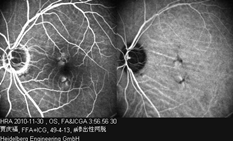
���ۣ�FFA�����ܿɼ���Ƭб������Ĥ���壬�ư����ɼ�Ƭ״ǿӫ�⣬���ڣ�����Ĥ���岻�䡣�ư���ǿӫ��Ƭ���У�ICGA�ư����ɼ�СƬӫ���ڱ�(ɫ�ضѻ�?)
Right eye: The dye transit was slightly retarded. There were multiple round-shaped, well demarcated hypofluorescence spots in the posterior portion of the retina, with no staining in the late phase. The margin of the optic disc wasblurred and was hyperfluorescen in the late phase. In ICGA, the hypofluorescence spots remained unchanged from the beginning to the end.
Left eye: FFA showed clusters of choroid folds in the mid-peripheral retina. Two hyperfluorescent spotsin the macular was shown in the early phase, laterthe hyperfluorescence gradually diminished.
�������
��������������Ĥ����
��������Ĥ����?
˫������Ĥ��©�ۺ�֢?
˫������������
Impression
Exudative retinal detachment OD
Choroidal detachment OD?
Uveal effusion syndrome OU?
Age-related cataract OU
�����鷿��¼
Discussion
�̳�������ҽʦ��
���ߵ��۷������������½������ڳ�����ǰ��Ӱ�ڵ����ۿƼ�飺˫�۾�״������»��ǣ��������ԣ��۵ף���������Ĥ��������λ�ı䣬δ����ѿף���Ϸ��ܱ߲��ɼ�һ��Ե�����¡����;���۵�����ͷ���̱ȴư���δ�������쳣������Ĥƽ���������۵ױ��֣�����Ϊ����������Ĥ���룬�۵���Ϸ�������¡����������������壬Ϊ�ų�ռλ�Բ��䣬����B�����ʳ�����CT��飬�����ʾ��¡���Բ���Ϊ����Ĥ���롣Ŀǰ��������Ϊ����������Ĥ����ϲ�����������Ĥ���룬˫�����������ϡ���������������Ĥ����ԭ����顣
Dr. Cheng Zhao-Hui
The patient had an onset involving only single eye and gradual progression . Eye examination revealed subcapasular opacity of the lens in both eyes with the right eye more affected. Fundus examination in the right eye showed retinal detachment shiftingwith the position and no retinal tear or hole was found. In the temporal-superior portion of the retina of the right eye, there was a localized protrusion blocked by nonclear optical media.The contralateral eye was normal except a relatively large cup. The above findings suggests exudative retinal detachment in the right eye. However, in order to exclude the possibility of any occupying lesion inthe temporal-superior portion, further investigation by B ultrasound scan, CDI and orbital CT are required for the patient. Theresults of these accessory examinations suggestchoroidal detachment.The diagnosis of this patientis exudative retinal detachmentcombined with localized choroidal detachment in the right eye and age-related cataract in both eyes. The cause of the exudative retinal detachment needs to be found out.
������������ҽʦ��
�û����۵�������ת��������Ĥ���룬���������Ĥ����⻬���Գƣ��̶����壬δ������Ĥ�ѿס����Ϊ����������Ĥ���롣����������Ĥ������һ�̷ּ�������Ĥ���룬��������Ĥ����Ĥ��������֢��Ѫ�ܲ��Լ�ȫ��ѪҺ��Ѫ���Լ��������䷢��������Ҫ������ĤëϸѪ�ܺ�ɫ����Ƥ���Ϲ����ܵ��ƻ�������Ѫ��������ĤҺ����������;ۼ�������Ĥ���γ�����������Ĥ���롣�û����۵ױ��ֺ��۵���Ӱ���ɻ����ų�������Ѫ���Բ������֢�Բ��䣬����ȫ����ʪ�Թؽ���1�꣬δ�ü������ƣ����۵�����֢�Ա��֣����ϵͳ��ԭ������ų���Ӧ��������Ĥ��©�ۺ�֢���ò��۵ױ���Ϊת��������Ĥ���룬����ԭ���Բ�����������빮Ĥ��֯�쳣���о������������йء�Ӧ�й�Ĥ��ȼ�⡣
Dr. Zhang Longli
The fundus examination of the right eye displayed shifting retinal detachment.The detached retina was smooth and symmetrical, with no fold or retinal hole. Exudative retinal detachment is usually secondary to retinal choroid tumor, inflammation, vascular disease or systemic blood and vascular diseases. The mechanisms relies on disfunction of retinal capillaries and the pigment epithelial barrier, leading to plasma and choroidal effusion and accumulation of fluid in the subretinal space. Based on the fundus examinations and FFA of the right eye, the possibility of tumor, inflammation or vascular disease could be excluded. Although the patient suffered from rheumatoid arthritis for one year, he was not on corticosteroidstherapy. There is no evidence showing the concomitant systemic disease is relevant of the fundus disease. The differential diagnosis also include uveal effusion syndrome, which is characteristic by exudative retinal detachment.The mechanism of uveal effusion syndrome is still unknown. It may be caused by scleral abnormalities or vortex venous obstruction. Measurement of the sclera thickness can help to establish the diagnosis.
������������ҽʦ��
����Ĥ��©�ֳƽ�״����Ĥ��©�����ط��Խ�Һ������Ĥ����״�������Ĥ����Ϊ�������ò�ԭ�������ٴ���Ϊ�ط��Ժͼ̷��ԣ�ǰ��Ϊ����������Ϊ����С�������������ֿɷ�Ϊ��Ĥ�쳣��Ĥ�������͡��ٴ�����Ϊ����λ�ƶ��İ���״����������Ĥ���룬�����۵��·������ѿ�����ѹ��������;����Ĥ����⻬��һ���̶����壬���ٷ�����ֳ�Բ���������Ĥ���䡣�۵�ӫ����Ӱ��������Ĥɫ����Ƥ�����ʱ���״����λ�ں�����Ⱦ����©��UBM���ɼ���״�������Ĥ���롣�û���������������������Ĥ��©��
Dr. Zhang Xiaomin
Uveal effusion syndrome is also known as ciliary choroidal uveal leakage, and is characterized by idiopathic serous detachment of choroid, ciliary body and neurosensary retina. Theetiology is stillunclear. Clinically it��s classified as idiopathic and secondary uveal effusion. The idiopathic type usually presents normal eyeball, whereas the secondary type is related to pure microphthalmia. The former type is further divided into two subtypes, one with normal sclera and the other with abnormal sclera. The clinical feature of this disease is shifting spherical or semiglobular retinal detachment, frequently involving the inferior portion of fundus. The surface of the detached retina is smooth, no fixed fold and rarely forms PVR. Angiographic feaures include leopard spot in the posterior portion of the fundus, corresponding to RPE proliferation. Staining and leakage are usually absent . Ultrasound biomicroscopy can detect ciliary body and choroidal detachment. The signs and accessory examination of this patient strongly indicate uveal effusion syndrome.
����������ҽʦ��
����������Ĥ��������ɶ����������(��1)�����������������ѹ����Ĥ�۴�����Ĥ�ȡ����⣬Ҳ���ڽ�������������ԭ������·������ۻ�˫���Է�������Ĥ���롣���������Ϊ�ط�������Ĥ��©�ۺ�����������߿��ܴ���������������㹮ĤѪ����չ��Schlemm���ڼ�Ѫ��Һ����ѹ�����������ɼ�����������ϸ��������Ĥ��Һ����λ�ı�ķǿ�Դ������Ĥ���룬����Ĥ��Һ�е��������Գ�������Ѫ��Ũ�ȶ����������Լ�Һ��������(���ڰ�������)���ٴ�����Ǩ�ӣ���������л������أ���Ƥ����̴�������лҩ�P��Һ��Ĥ�۴������������Է�Ӧ��
�ò�DZ�ڷ������ƿ��ܹ�Ĥ���о��������쳣��������Ĥ���������쳣���ڳ�����ദ���ְ�㹮Ĥ�п����г����о�����ѹ������Ч���������Ͼ�״�峬���黯�Ա������н�һ������۵ס�
Dr. Li Xiaorong
Exudative detachment of the choroid and ciliary body may be caused by a variety of disease states(Table 1), eg, postoperative hypotony, scleral buckling procedures, scleritis, etc. In addition, it may occur spontaneously with no apparent cause in one or both eyes of healthy individuals. These patients are defined as having the idiopathic uveal effusion syndrome.
In this latter group of patients other findings which may be present include: dilation of episcleral blood vessels, blood in Schlemm's canal, normal intraocular pressure, few vitreous cells, nonrhegmatogenous retinal detachment with shifting of subretinal fluid, elevation of subretinal fluid protein to two or three times the normal plasma level, elevation of cerebrospinal fluid protein (50% cases), protracted clinical course with remissions and exacerbations, and poor response to treatment with corticosteroids, antimetabolites, drainage of subretinal exudate and scleral buckling.
Its underlying cause was a congenital anomaly of the sclera and vortex veins that resulted in intermittent obstruction of the flow of the venous outflow of the posterior uveal tract. It may be helpful by multiple segmental equatorial partial thickness sclerectomies and sclerostomies with decompression of the vortex veins. Besides, the cataract was severe in the right eye, phacoemusification and intraocular lens implantation should be combined with the UES surgery in order to facilitate further examination of the fundus with BIO.
�������ƾ���
Treatment and Outcome
2010��12��8�գ����۹�Ĥ̽��+��Ĥ������+�����ϳ����黯������+�˹���״��ֲ����
���У�����Ĥ�ɰ�ɫ��������¡����¹�Ĥ������������Һ��������ȡ���ֹ�Ĥ��֯�Ͳ������
�����1�죺Vod 0.15��IOP 8.8mmHg;Vos 0.6��IOP 9.1mmHg�����۵���Ϸ�����Ĥ¡��ȼ�С���·�����Ĥ������������½���
����1�ܣ� Vod 0.15��IOP 5.5mmHg;Vos 0.6��IOP 8.1mmHg��������Ϸ�����Ĥ���������ʧ���·�����Ĥ������ȼ��١�
The right eye underwent operative scleraexploration combined with sclerectomies. Phacoemusification combined with IOL implantation was performed simultaneously.
A piece of sclera tissue was collected during the operation for pathologic examination .
PE on the first daypost-operation:
Vod 0.15��IOP 8.8mmHg;Vos 0.6��IOP 9.1mmHg
The choroidal detachment in the temporal-superior portiondecreased in size. The retinal detachmentimproved.
PE at one week post-operation:
Vod 0.15��IOP 5.5mmHg;Vos 0.6��IOP 8.1mmHg
The choroidal detachment disappeared and the subretinal fluid further decreased.
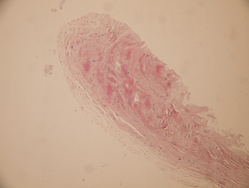
ͼ7 �������������Ĥ��ԭ���������ܰ�ϸ������
Fig7 Pathologic results showed focal lymphocytes infiltration.
��һ������Ĥ��©
TABLE 1: UVEAL EFFUSION
|